There have been several attempts within the robotics community to come up with cheaper and more portable surgical robots. Several of these could be real contenders to the dominant da Vinci Surgical system technically, however the strict medical regulations complicate the road to the operating room.
One machine in particular that is worth mentioning is the RAVEN II Surgical robot. Initially developed with funding from the US military to create a portable telesurgery device for battlefield operations. This impressive looking machine with it’s two wing like arms is valued at $200.000 so it represents almost a 90% cost reduction in comparison to the Da Vinci, but it also represents a different mindset entirely. All of the software that is used to control the RAVEN II has been made open source, meaning that other people could use and improve it or re-appropriate it to fit their needs. Currently there is only so much need for very specific surgery robot control software, however what it means is that this system is very useful to researchers in universities to test new ideas and software approaches to robotic surgery. The tradeoff is that it might take a while before the RAVEN II will be fully embraced by regulatory and commercial worlds - if ever. The Raven unfortunately doesn’t have the required (and often costly) safety and quality control systems in place, required by regulation to allow it to be used on humans.
Although the story of the RAVEN II is inspiring, $200.000 makes that it would likely still be out of reach for most medical hacker communities. So in order to test the plausibility and preferability of such an endeavor, for the past five months I have been trying to build a DIY surgical robot for around $5000 by using accessible prototyping techniques like laser cutting and 3d printing and by sourcing as many ready-made parts as I could find.
After consulting with experts from the medical sector as well as with roboticists it became clear that there are three major challenges to the design of a surgical robot, (theoretically) capable of performing laparoscopic surgery. Firstly there are the tools: during a single operation a surgeon would switch between various types of tools, so a robot would either have to have many of them or they should be able to be interchangeable. Furthermore the instruments used in laparoscopic surgery are extremely small, so making them yourself would be a big challenge. Secondly, there is the fact that anything that comes into contact with the human body has to be sterile to reduce the risk of infection. In hospitals therefore most tools are stainless steel so that they can be sterilized by placing them in an autoclave. A bulky machine that uses high pressure and hot steam that is not very likely to be accessible to many people. Thirdly there is the type of motion a surgical robot should be able to make, whereby a fixed point of rotation in space is created where the tool enters the body through an entry port - or 'trocar'. The trocar needs to be stationary so as to avoid tissue damage.


As it turns out it is in fact really easy to buy laporoscopic instruments online. After a few unsuccesfull attempts at getting some shipped over from the US by ordering from Ebay, I switched to using Alibaba, where you can order them directly from their Chinese manufacturers. For around $40 a piece + shipping they can even be shipped in sterile packaging if required. The fact that you can order directly from the manufacturer also makes sure that you can have a steady supply and order different types of instruments. So not only could you base a design off of them, it also means that you could simply dispose of the tools after use and order new ones. Besides selling laparoscopic instruments, many companies on Alibaba even sell fairly affordable peripheral equipment required for surgery, like monitoring equipment, camera modules and CO2 insufflation pumps for example.
Another realization during the staring phases of the project was that you could simply re-appropriate domestic devices to account for not having access to hospital infrastructure. A simple domestic oven turned to 160 degrees centigrade for 4 hours, would be a simple alternative to an autoclave, and for plastic parts you might even be able to use a microwave.
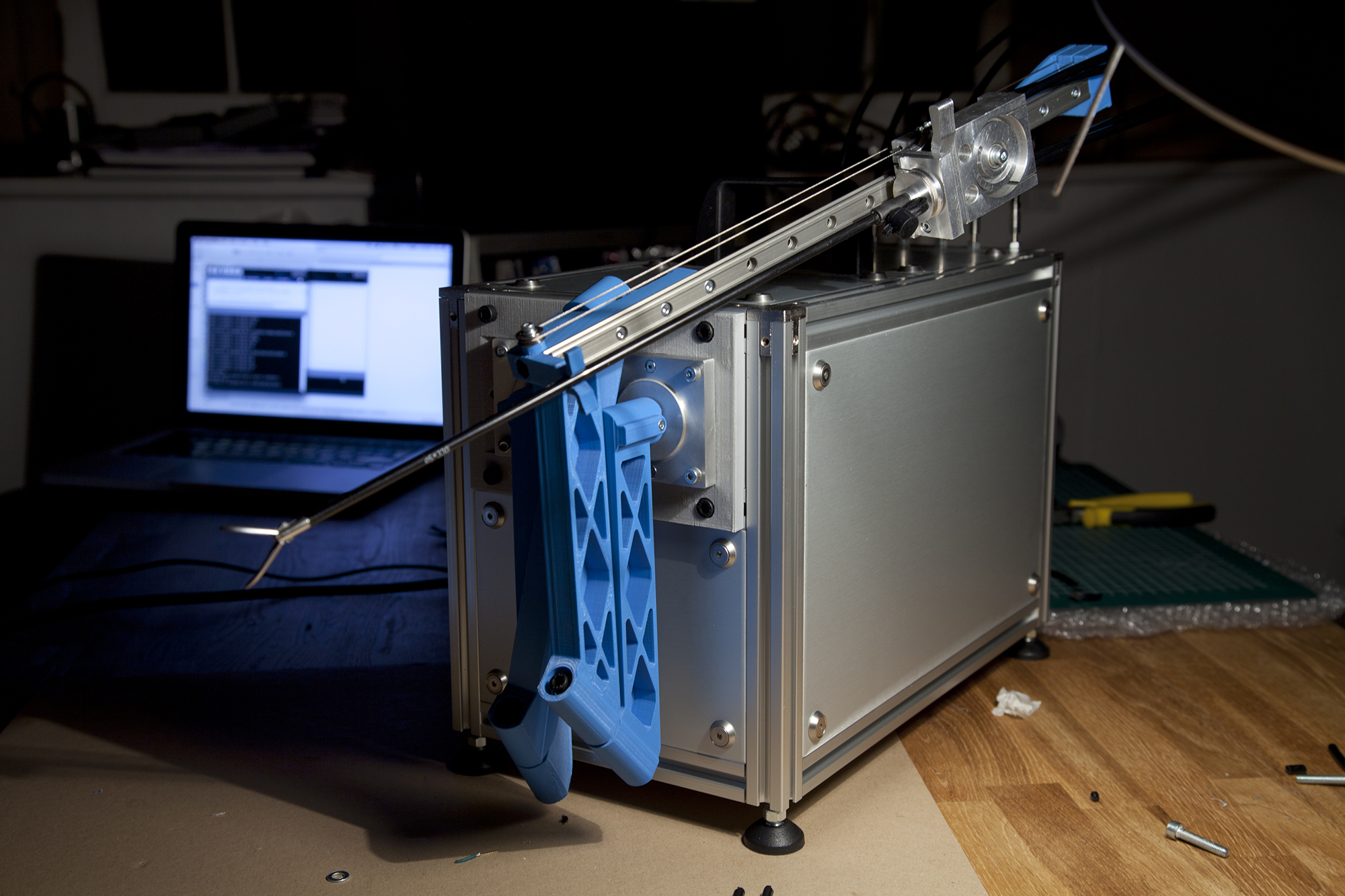
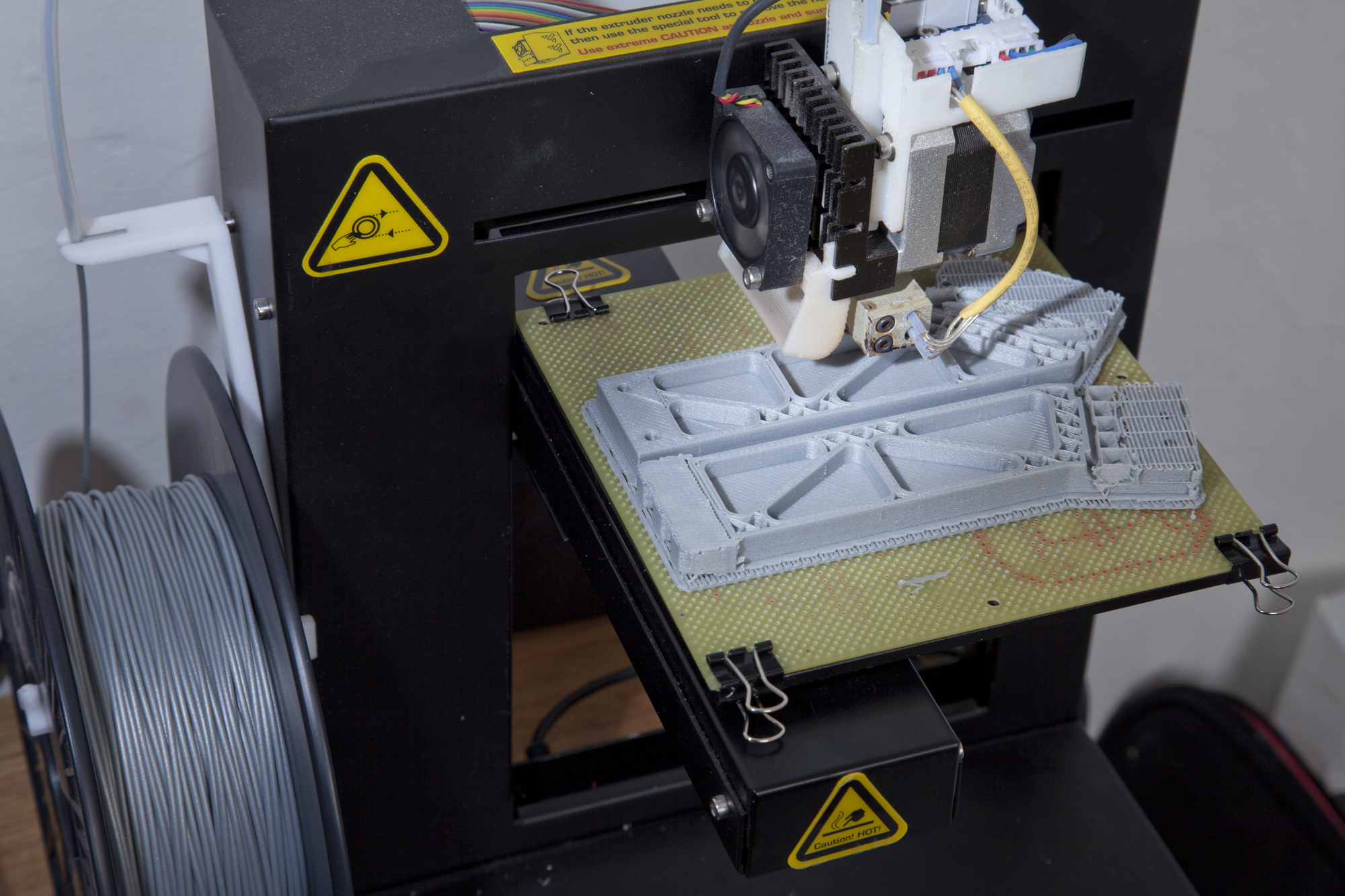
So as it turned out designing the mechanical system was actually the most complicated part of the process as it required lots of iterations. Working my way through some of the more conventional solutions I ended up with a design that uses four 3d printed parts controlled by two DC servo motors that rotate around a central pivotal point.
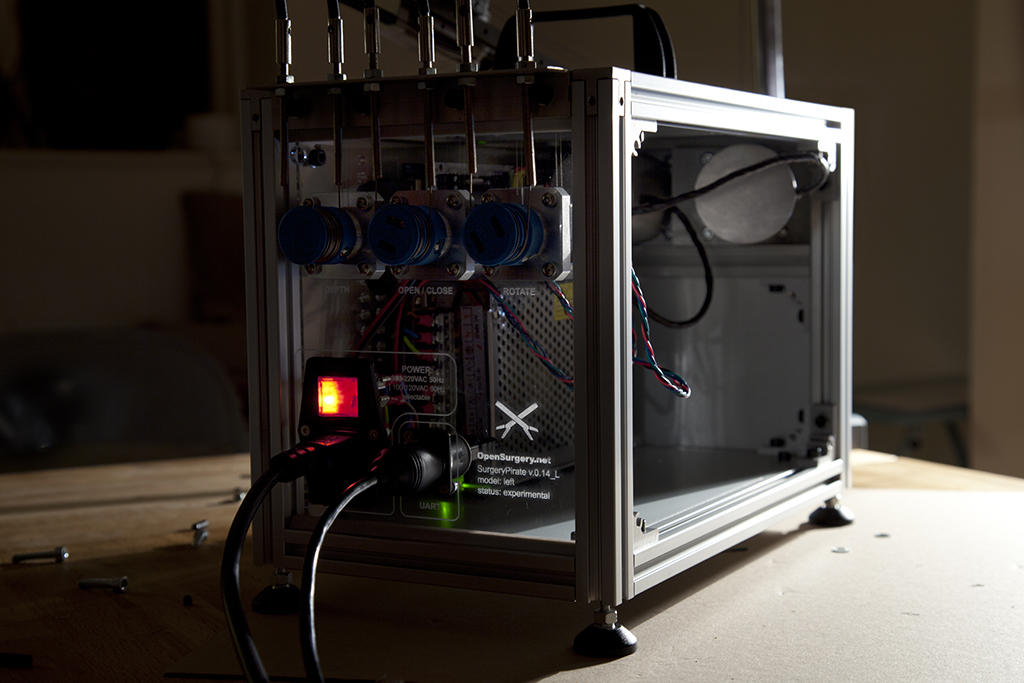
The electronics to control the robots are pretty much copied directly from designs used in 3d printer communities. The reasoning behind this is that this would not only increase the availability but also community support when needed. The software in turn was build with Processing - the famous open source scripting language - for the same reasons.
Although I wouldn’t recommend to attempt surgery with it just yet, after five months of iteration it does in fact move. And based on my experiences the concept of a DIY surgical robot is surprisingly plausible. If you would be able to build a community of makers who bring the same amount of attention and dedication to building surgical tools as they do to designing 3d printers and cnc machines these days, I believe accessible DIY surgery equipment would be within reach.
The biggest limitation is that you would still require a trained surgeon, or someone with extensive knowledge of the human anatomy and knowledge of surgery, to perform the operation. However I don't think it is to hard to imagine that there would be surgeons who share in the same ideology and become part of such communities.
The legality of that however remains questionable and it’s preferability off course debatable.